Table of Contents
Introduction
Chapter 1: Basic Understanding
What is Obesity?
Diagnosis ?Body Fat Ratio
Causes of Obesity: Disturbed Metabolism and Vicious Cycles
Six Factors of the Vicious Cycle of Obesity
Who Suffers from Obesity?
What are Sensible Weight Control Methods?
Obesity and Diabetes: Siamese Twins
Chapter 2: Consequences of Obesity
Complications and Related Diseases
Obesity’s Affect on Social and Sexual Life
The Vicious Cycle of Obesity
Chapter 3: Currently Available Weight Control Methods
Fasting
Selective Diet
Medication (pills and drugs)
Herbal Products and Dietary Supplements
Weight Loss Machines
Surgical Procedures
Criteria for Judging Sensible Weight Control Methods
Chapter 4: A Sensible Combination of Four Weight Control Methods
Stress Management
Sensible Eating Habits
Sensible Exercise
Metabolism Boosting Dietary Supplement
Chapter 5: Eleotin-Mb A Dietary Supplement for Basic Metabolism
How was Eleotin-Mb Developed?
How does Eleotin-Mb Work?
What Happens when Underweight People take Eleotin-Mb?
Weight Recovery
Is Eleotin-Mb Safe?
Any Side Effects or Drug Interactions?
How do you Prepare and Take Eleotin-Mb?
Balanced Eating Habits
Can Alcohol be Consumed with Eleotin-Mb?
Does the Body Develop any Resistance to Eleotin-Mb?
How long Should I Take Eleotin-Mb Before the Effects Start?
Eleotin-Mb and Diabetes
Improved Sexual Energy
Improvement of Sleeping Quality
Why is it Named Eleotin-Mb?
Eleotin-Mb Evaluated Against the Criteria for Judging a Sensible Weight Control Method
Additional information
Appendices
Appendix 1. Comparison of Current Weight Control Methods
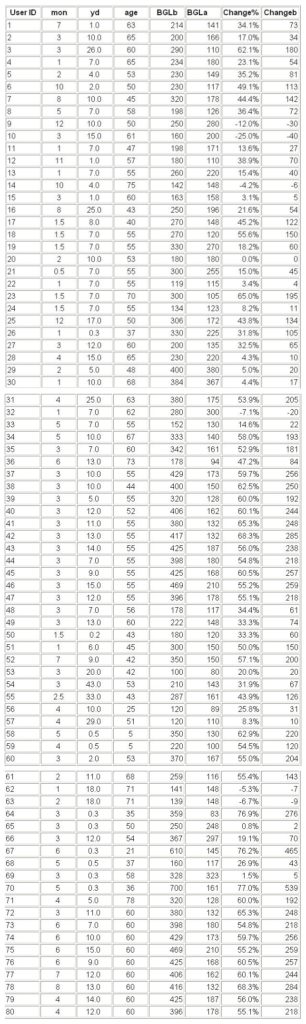
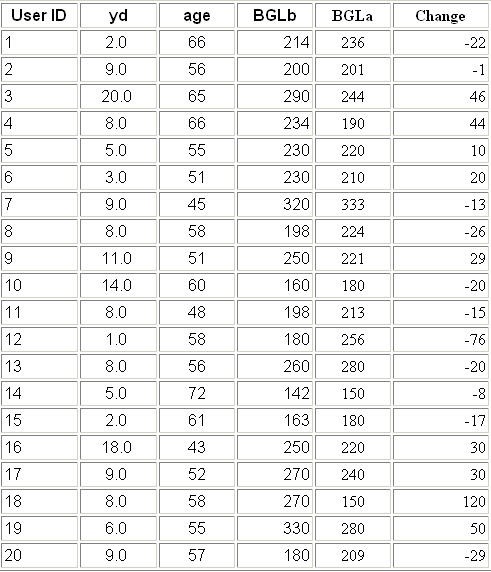
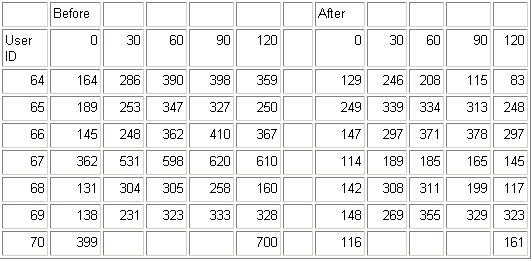
Appendix 2. Eleotin-Mb Weight Control Effects (1)
Appendix 3. Eleotin-Mb Weight Control Effects (2)
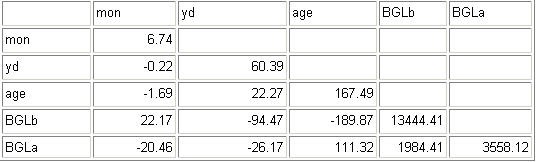
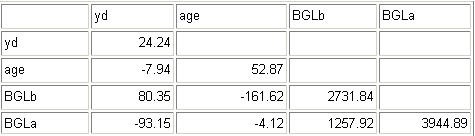
Appendix 4. Mechanisms of Action of Eleotin-Mb
Introduction
More and more people are becoming concerned about their weight. Looking at recent obesity trends, they should be. More than half of North American adults are considered overweight today, and obesity analysts believe that the clear majority of Americans will become overweight within the next ten years. In other parts of the world, obesity is growing at a less alarming rate but is still prevalent. Worldwide, medical experts are now strongly warning their patients that obesity is a leading contributor to numerous long-term health threats. How can we slow or stop the progress of this alarming trend?
Of course, there are many weight control methods. Some methods appear to be quite innovative. There are programs like the diet cafe, diet package tours, fasting clinics, vegetable enzyme diet, one fruit diet, emperor’s diet, the protein diet etc. Yet, obesity is still spreading rampantly. The emergence of all of the above novel weight control methods is really just a sign of our frustration and willingness to try anything, rather than of the effectiveness of those methods.
Since society places such a huge premium on physical appearance, the demand for weight control products is enormous. The Weight Loss Industry understands that people are very desperate for a weight control product they can believe in. So numerous innovative products are introduced each year. Many people try these new products and spend billions of dollars each year. However, few people succeed at losing weight and those who so succeed initially tend to gain back the weight rapidly. These 뱘o-yo?customers are highly regarded by the Weight Loss Industry because they become repeat customers.
Isn’t it time we question why all these weight control methods always fail to deliver their promises? We need to discover what went fundamentally wrong. We need to understand what our realistic weight loss options are and the chances of achieving them. We believe that presently most people take a very simplistic approach that focuses only on how many pounds of weight they lose. As long as everyone focuses on the poundage lost, there is no way to solve the obesity problem. We must look deeper into how someone both gains and losses weight. Then we will be closer to the answer.
We believe that what we should not be very concerned about how many pounds are lost. Rather, we should focus on correcting the imbalance of the basic nutritional and energy metabolism that started the whole weight gain problem in the first place. We believe that focusing only on lost poundage is wrong and even dangerous. This narrow focus can often lead to using superficial weight loss approaches with many dangerous side effects, with only temporary weight loss results, and with an unrealistic chance of success.
We wrote this booklet to remove the many misconceptions and misunderstandings regarding weight control. Inside, the pros and cons of various weight control methods are compared and presented as objectively as possible. Also, we provide some basic scientific principles of how weight gain occurs and how to lose and control weight. Lastly, this book introduces information about a newly developed product called Eleotin-Mb, which has recently became popular in North America and Japan.
Chapter 1: Basic Understanding
What is Obesity?
Obesity is a state of being overweight, or having excessive fat. In medical terms, obesity is defined as having excess adipose (animal fat) tissue deposits. Alternatively, obesity means that the weight ratio of fat to total body mass exceeds 25% for men or 30% for women. On average, the normal ratio is around 18%.
Does a lower fat ratio mean a healthier, better body? While for most people this is true, the answer is not always yes. To keep a healthy body, we must maintain a certain fat level. Maintaining an excessively low fat ratio is not healthy. A normal and healthy fat ratio is around 18%. The human body largely consists of bones, muscles, and fat. The bones and muscles play the role of sustaining the body structure and its daily activities. Fat’s primary role is to store excess energy for use on a rainy day. Fat also constitutes an important part of our vital organs. Our brains, for example, is composed mostly of fat. When we are sick and the proper level of energy and nutrition is not supplied, body-fat begins to get disintegrated, becoming an alternative source of energy and nutrition. Therefore, when the fat ratio is too low, our body is exposed to the danger of not having enough reserve energy during a period of insufficient calorie intake (e.g. serious illness). Also, an insufficient fat supply hinders the formation of certain vital organs. The fat is usually 3%-5% of your total body weight. Fat is an important building material for many other key organs of the body. This is why simplistic fasting and extreme dieting often harm our body permanently. Body-fat itself is not harmful. Excess body-fat is harmful but insufficient body fat is equally harmful.
Diagnosis ?Body Fat Ratio
Men and women are considered obese when their body fat exceeds 25% or 30% respectively. However, measuring a person’s exact body fat ratio is not as easy stepping on some scale. So, for convenience, people can use the following methods:
1) Standard Weight Index: Normally, the standard weight is computed as (height in centimeters – 100cm) times 0.9. For example, for a person who stands 170cm, the above calculation is (170-100) * 0.9 = 63kg. Therefore, 63kg is the standard weight for a person whose height is 170 cm. If a person’s actual weight exceeds the standard weight by more than 20%, he is considered overweight. Degree 1 obesity is weighing 20% more than the standard weight. For the person above whose standard weight was 63 kg, he is Degree 1 obese if his weight is more than 75.6kg. For Degree 2 obesity, he should weigh more than 81.9kg, which is 30% over standard. Degree 3 obesity is 40% higher than the standard weight and Degree 4 obesity is 50% higher and so on. This method is relatively easy to use. But, this method does not really distinguish between a sturdy physique and someone who is overweight. In other words, according to this method, a highly trained body builder is equally classified with someone who is more overweight.
2) Body Mass Index: The body mass index is a ratio of one’s weight in kg to the square of your height in meters. For example, a person with a height of 170cm and a weight of 65kg, the body mass index calculation goes like 65kg/1.7m*1.7m=22.49. For this person, 22.49 is their body-mass number. Experts use the index to classify people. People with a body-mass number of 20-25 are considered normal, those between 25-29.9 are overweight, and those over 30 are labeled as obese. This is again a relatively simple method, it has the same weakness as the above standard weight index.
3) Skin Pinching Test: This method uses a compass-like skin-fold measurer to measure the skin-folds of the biceps and triceps. When used on triceps, obesity is defined as skin folds of more than 3cm for women and 2cm for men. This is a reasonably accurate test that should be available through you physician.
It is true that for most people determining who is fat and who is not fat is a relatively straightforward task. Therefore, for most of us, we do not need such sophisticated methods as described above. But, remember there may be some psychological dimensions to the obesity problem. For example, some overweight individuals can deny their problem. They maintain they are not 몋hat?overweight. For these people, and for everyone else who enjoys calculating some weight ratio numbers, we hope you like the above calculations. But, for the rest of us, these calculations are just academic since we already know our weight situation.
Causes of Obesity: Disturbed Metabolism and Vicious Cycles
Obesity starts when something goes wrong with our basic nutrition and energy metabolism. Through our basic metabolism, nutrients are taken in, digested and transformed into energy to fuel our activities and maintain basic biological functions such as breathing. Carbohydrates that are consumed are digested and turned into blood sugar, which is the fuel for human activities and basic biological sustenance. Healthy people maintain a balance between the nutrition intake (the fuel) and its usage (cellular burning of the fuel). As long as there is a healthy balance in this basic metabolism, one does not become overweight.
However, once something goes wrong your basic metabolism, the vicious cycle of obesity gradually sets in. Here is an example of the typical stages of damage that occurs to a person’s basic metabolism:
Stage 1 – Constant overeating leads to high blood sugar levels and over time the unused blood sugar is converted into body fat. At the same time, high blood sugar levels require the body to produce larger quantities of insulin to process the high blood sugar. Insulin is a hormone that helps transfer the blood sugar from the blood system to the body’s cells.
Stage 2 – After several years, the body’s ability to produce insulin has diminished considerably. During this time the body also reacts very negatively to the prior excessive production of insulin and the body begins to use insulin less efficiently. Thus after several years of high blood sugar, insulin production becomes weak and your body also becomes resistant toward the insulin it produces. Once, the insulin balance is disturbed like this, the body has one fewer weapon to fight against obesity.
Stage 3 ?Numerous years of this vicious cycle of obesity can lead to numerous medical complications with diabetes and heart disease being the most common.
To summarize the vicious cycle can be seen as 1) Habitual overeating that leads to 2) high blood sugar and long term high blood sugar which leads to 3) insulin insufficiency and insulin resistance. Insulin insufficiency and insulin resistance leads to diabetes 4) diabetes and other major complication that lead to a still higher blood sugar levels.
In fact, there are several dimensions of this vicious cycle of obesity. In the above example, even though the individual is overeating, the person’s cells may still receive insufficient fuel (blood sugar). How can this happen? Since insufficient insulin was released, the excessive blood sugar of the overeater remains in their blood stream. Therefore, their cells cry to the brain for more energy/nutrition. The brain interprets this signal as a demand for more food and the individual will feel a need to eat more. Additional overeating starts another cycle.
In sum, in the vicious cycle of obesity, eating more leads to eating still more through a few well-known mechanisms. As long as the disturbed basic metabolism stays unfixed, the basic energy metabolism tends to get worse and worse. Somehow, one must cut this vicious cycle, and rehabilitate the body뭩 basic metabolism. Remember, the quicker you stop this vicious obesity cycle the better. Prevention is always preferred. In order to prevent obesity, one has to be aware of those factors which lead to obesity.
Six Factors of the Vicious Cycle of Obesity
There seem to be about six factors that start the above mentioned vicious obesity cycle:
1. Poor Eating Habits – Overeating obviously starts and aggravates obesity. This does not require too much explanation. Just look around. Modern men and women simply eat too much and too often. However, it is no only quantity of the food consumed but also the quality. It is noteworthy, that the lack of some important nutrients also leads to obesity. Partial malnutrition leads to obesity too. When certain nutrients are insufficient due to an unbalanced diet, our body continuously demands those insufficient nutrients, and more often than not this leads to additional overeating. You would be surprised to find out how unbalanced a fast-food meal is or how few nutrients are contained in all junk food. If one relies on junk food for even 15% of your food consumption, it can lead to serious obesity and malnutrition at the same time.
2. Environmental Factors ?Our way of living is constantly changing, new environmental changes are introduced daily. For example, Chinese people used to drink a lot of tea. Tea, in general is extremely healthy, and contains some very important nutrients. Now, soft drinks like Coke-Cola have saturated the Chinese market and are massively consumed. It is no wonder that the obesity problem in China has increased. Another simple example would be more automobiles lead to more obesity. Also, we believe that more computers will lead to more people spending their time in front of a screen rather than moving around. More obesity will definitely result from more computers. If we look around, whenever there is a change in our life style toward more convenience, it almost always leads to more obesity. This is a tragic price we have to pay for modernity.
3. Drug Side Effects – Medications like birth control pills, antihistamine medications, asthmatic and allergy pills may also be a cause to obesity. These drugs are quite frequently used. Therefore, most of us have been exposed to the danger of obesity from the side effects of these drugs. As a principle, any drug that causes a change in your hormone balance tends to lead to obesity. We should know that gaining weight is one of the most common side effects of all the drugs. Some herbal products also have weight gain side effects because they stimulate appetite. We tend to underestimate the seriousness of obesity related drug side effects. The obesity caused by drug side effects is harder to handle than the obesity caused by other factors. Thus, we have to pay extra attention to the drug side effects related to obesity .
4. Genetic Factors – When parents are overweight, the chance of children being overweight is as high as 50-70%. When parents are overweight, children should be very careful. Recently, scientists have claimed to have found the 밼at genes? In theory, this is fantastic. Wouldn’t it be fashionable to blame everything on certain 밼at genes? This would be great because then no one has to feel guilty and the solution sounds simple to fix. Although promising, it will take numerous years until a miracle gene therapy safely blocks the culprit fat genes.
5. Psychological Factors ?Stress can cause people to overeat. Such compulsive eating surely contributes to a person뭩 obesity. Also, stress adversely affects the hormonal balance and becomes a contributing factor to obesity. Other, more serious psychological problems like depression can also lead to overeating. If this is an important factor in your situation, we recommend that you seek expert guidance to ensure that this factor is minimized.
6. Hormone Disorders – As was just mentioned, any hormone disorder can cause obesity. Some argue, quite controversially, that hormone disorders are very rare and only apply to 1% of obesity patients. As pregnancy hormonal problems can lead to large permanent weight gain, we do not agree with this assessment. However, as not much is known about this cause, we are unable to substantiate this belief.
Who Suffers from Obesity?
In affluent countries, obesity is more prevalent. Of course, in North America, the obesity problem is very serious. In Canada, 30.5% of the total population suffer from weight problems. The above figure when further segregated is more startling. Over 50% of all adults in Canada are considered overweight. The situation is no better in the U.S. In 1996, there were also more overweight adults than normal adults. In 1996, there was an estimated 70 million people who were overweight. Due to the steep growth rate and pervasive effect on all age categories, U.S. obesity forecasts are very pessimistic. Some forecasts indicate that within 20 years, a clear majority of all Americans (65%) will be overweight if nothing is done. Nobody, it seems, is safe from the threat of obesity.
What are Sensible Weight Control Methods?
It is important that 몏eight control?methods should be sensible. Weight control methods should be about more than simple weight loss. They should focus on a method to normalize the person’s metabolic balance, and as a result they should provide weight loss. Weight loss at any cost is a wrong approach and always very dangerous. Let’s take the example of a glamorous weight control method called 멿iposuction? This is an extreme weight control method that works by directly removing body fat out of a person’s body through a surgical operation. Of course, the immediate consequence of this surgery is that your body weight is declined, and your body fat ratio is reduced. However, there are very serious side effects from this operation and the initial weight loss tends to return very quickly. This surgical operation does not address the fundamental causes of weight gain it simply an quick way for individuals to experience a large loss in weight. Of course, the fat comes back quickly. In order for a weight control method to have real and long lasting benefits, that weight control method should contribute toward the normalization of the basic nutrition and energy metabolism. There is no other way. Basic nutrition and energy metabolism is where the problem started. Therefore, that is where the solution must be found.
Obesity and Diabetes: Siamese Twins
Diabetes and obesity are so closely related that many experts say that obesity and diabetes are like two sides of the same coin. That is, these experts feel that any discussion about obesity must include a discussion about diabetes because they are so similar. It is little wonder that many obesity specialists are also diabetes specialists. Let’s review their similarities. Diabetes results from a metabolic imbalance that is very similar to obesity. Diabetes is a disease that results from 1) Insulin not being produced or secreted properly, 2) an increase in insulin resistance. The outcome is high blood sugar, which will result in body fat increase. The second similarity is that diabetes and obesity are highly correlated. That is, 75% of all obese individuals also suffer from diabetes. Obesity can often trigger diabetes and diabetes can lead to obesity. Diabetic patients should be extra careful about their weight and obese individuals should take preventative steps due to their high likelihood of becoming diabetic. Diabetes disarms an individual of the weapons to fight obesity and obesity worsens diabetes. There are so many similarities between them that doctors refer to the two as Siamese Twins. Also, experts agree that if there are permanent solution to diabetes, it must be also permanent solution to obesity, and vice versa.
The discovery presented in this book, Eleotin-Mb, was originally based on diabetes treatment called P-700. The Julia Macfarlane Diabetes Research Center (the University of Calgary) developed the P-700 diabetes treatment. The P-700 treatment was shown to naturally and safely control blood glucose levels. After a six-month usage of P-700, diabetic complications were reduced and the reduction was maintained semi-permanently. This diabetes treatment technology has been licensed to Eastwood Bio-Medical Research Inc. since January 1998 under the brand name – Eleotin A, B, and C. When Eleotin was reported to the American Diabetes Association, one of the world’s leading diabetic scholars suggested to Eastwood that they should apply the Eleotin technology to develop a weight control product. His reasoning was that since Eleotin provided semi-permanent diabetes protection and control, it would also be successful at providing long lasting weight loss. As we explained earlier, diabetes and obesity are two sides of the same coin. The improvement and control of diabetes naturally requires weight loss if that is a contributing factor to the diabetes. Therefore, Eastwood began to review how the Eleotin technology could be amended and developed into an effective weight control product. Based on the recommendations of the American Diabetes Association and the University of Calgary, Eastwood completed its analysis and review and a new weight control technology has emerged. From the original diabetes treatment technology, Eleotin, primary hypoglycemic ingredients (blood sugar lowering ingredients) were removed, and metabolism-boosting ingredients were added. The result was the creation of Eleotin-Mb.
CHAPTER 2: Consequences of Obesity
Complications and Related Diseases
We are constantly told how bad obesity is. Well, let뭩 just repeat the reasons one more time.
Obesity is dangerous because it is directly and indirectly related to so many diseases.
1. Coronary Diseases – Experts say that obesity is one of the leading causes of heart disease. The fat deposits around the heart continue to burden the heart muscles forcing them to work harder. This additional workload increases the individual’s chance of various heart diseases. The fat deposits accumulated around the abdominal region also increase the likelihood of heart disease, as well as, diabetes. Excess fat accumulation in the veins and arteries imposes an obstacle for smooth blood-circulation. Severe capillary troubles are the eventual result as blood cells clogs and capillaries break. If this happens in the brain, it is called a stroke and it can result in permanent paralyses and death. Obese people have a 75% higher chance of suffering a stroke than other people.
2. Diabetes – We have already explained diabetes. So, let’s just say that the correlation between obesity and diabetes is so close that many experts regard these two as Siamese Twins. The correlation is approximately 75% of diabetic are also obese. Diabetes is called the disease of diseases?because it is a major contributor to so many other diseases. Diabetes can lead to blindness, kidney disease, heart disease, infections and amputations,. Obesity and diabetes make a lethal combination.
3. Liver Diseases – Obese people often develop fatty livers. Fatty livers can develop into liver cirrhosis the hardening of the liver. Also, these individuals more readily have gallstone problems. Medically this is called cholelithiasis. In other words, obesity can often develop into a fatal liver disease.
4. Pregnancy Related Disorders – Hormonal imbalance caused by obesity may bring about serious pregnancy related disorders. Also a woman’s pregnancy may cause a disruption her hormonal balance that leads to excessive weight gain during the pregnancy. These disorders are not difficult to understand intuitively if we consider how many hormones are intricately interrelated during the whole process of pregnancy. Obesity is never good however obesity becomes particularly harmful during pregnancy. Also, some women never regain their hormonal balance after pregnancy. They will find it extremely difficult to loss their additional pregnancy poundage.
5. Bones and Joints ?Being overweight will creates pain in the lower back, knees, and ankles. These organs are created to sustain only a certain amount of weight. Obviously, constant and excessive weight can cause problems in these joints. Experts believe that many forms of arthritis are caused or worsened by the person being overweight.
We could continue to provide more examples as there is a very long list of complications and diseases resulting from obesity. However, we believe you now fully understand our point on the grave danger of being overweight.
Obesity뭩 Affect on Social and Sexual Life
Even though beauty and attractiveness are quite a subjective matter, obesity can hardly be seen as an improvement to a person몊 appearance.
It may not be politically correct to state that being overweight is not attractive but that is why there is such a demand for weight loss products. Why do people feel less attractive when they are overweight? Some concrete physical reasons we will provided. Why do people easily lose their confidence if they feel they are overweight? There are many theories why our confidence is affected by how we perceive our physical appearance. Finally, why does being overweight seriously affect a person’s social and sexual life in so many ways? Regardless of the theories, the general consensus is that being overweight puts a large strain on our confidence and can lead to many behavior changes. These changes in thoughts and behavior impact our social and sexual lives.
People feel less attractive for many reasons. There are many physical reasons which will cause a person to feel unattractive. Obese people’s physique appears very soft and slouched down. Since fat sags, men’s chest and belly sinks down. Females suffer from the sagging in the lower abdominal, hips, and thighs. When fat is accumulated in the skin layer, it induces skin expansion. If skin is expanded beyond its capacity, skin rips. In areas where fat is easily accumulated such as, lower abdominal, hips, thighs, and calves the skin is most prone to rips first. It is wrong to think that only pregnant women have this skin-tearing problem. Many overweight men and women suffer even more.
Obese individuals also have a greater body odor problem. All areas where flesh meets flesh such as the groin, arm pits, and toes can start to smell. Air is not able to circulate in such areas and skin diseases such as eczema and athlete’s feet occur, leading to odor. The problem becomes more serious especially in the summer time. Sooner or later, obese people themselves become very conscious of this odor problem. Naturally, individuals suffering from the above physical consequences of obesity can begin to lose confidence in themselves. They develop a very negative self-image in themselves and it starts to dramatically affect their thoughts and behavior.
For example, let’s examine how obesity can affect teenagers. Teenagers who are very overweight develop oversized knees and ankles to support their weight. This leads to bad walking postures and unattractive physiques. Overtime they develop very negative self-images. Also their learning ability at school can be affected. When too much fat becomes stored in the blood system, blood circulation is aggravated. The poor blood circulation can cause drowsiness, fatigue, and the appearance of laziness. If the blood flow to the brain is also aggravated or slowed, the teenager’s memory capacity may start to weaken and concentration becomes more difficult. Naturally, many of these teenagers start to avoid or limit relationships with friends and their school life also suffers.
Many adults also suffer from serious social setbacks due to their obesity. Quite often they are discriminated in some manner at work because obesity is often regarded as a sign of laziness. This seems to raise the standard for obese individuals. They had better ensure their work rate does not fall or they will become labeled as non-productive. However, if their confidence level drops, they may begin avoiding social and business contacts with co-workers. They may feel less confident in their ability to handle their work stress. This in turn further aggravates other aspects of their life (home life or physical fitness). This is yet another possible loop in obesity’s vicious cycle. Obesity makes people lose confidence, they go out less, less become even less physically active, they eat more when depressed and, they become even more obese.
Obesity does not help a person’s sex life either. Fat accumulated in sexually sensitive spots usually reduces their sensitivity to stimulation. Consequently, obese people lose interest in sex. Also, their poor physical stamina is a further deterrent to their sex life. Since they are more likely to be tired, they are less interested in sex. Sometimes the individual’s sexual confidence is another deterring factor to sex. They are more conscious of how their partner may be reacting to their weight. Sometimes serious cases of fat deposits may even make intercourse itself impossible, as the sexual organs are planted too deeply in the flesh. Through these and other processes, obese people become more and more distanced from sex. Male impotency is very prevalent among obese males. Especially, for a male diabetic, almost 50% of them become sexually impotent within 5-7 years. Erections become impossible due to the capillaries being blocked and other nerve damage. Thus being overweight can have a profound effect on how both we and others view ourselves. This in turn, impacts on our on our social and sexual lives.
The Vicious Cycle of Obesity
Obesity does not heal itself. Once the underlying mechanisms of obesity start, they seem to continue and intensify unless something is done. For example, most statisticians understand the difficulty of impeding or correcting obesity when it begins. Thus the most important statistical factor to explain future obesity levels is previous obesity levels. They understand that obesity intensifies its hold, and that once obesity is in the system, it persists. We also realize that becoming older does not seem to improve our obesity. This is a large concern since the rate of obesity in children is growing at a dangerous pace. Left alone, obesity does not go away and it usually gets worse. Therefore we must be very concerned. It may start out as a very mild and simple thing. People may tell you, don’t worry, you are still OK? You yourself may want to believe it too. But, sooner or later, your condition becomes more severe and serious. That is why it is so dangerous.
There are a few loops through which obesity intensifies itself. Insulin resistance, appetite induced by partial malnutrition, activity aversion, etc. Something sensible and fundamental should be done to the basic energy metabolism. Otherwise, obesity can only get worse.
CHAPTER 3: Currently Available Weight Control Methods
Currently there are 6 groups of popular weight control methods:
1) Fasting
2) Selective diet
3) Medication
4) Herbal products
5) Machines
6) Surgical methods
Let us look closely at each one of them.
1) Fasting
There are two types of fasting. One is pure fasting where you do not eat or drink anything except for water for a certain period of time. The period ranges from one week to 15 days. The other fasting method is to take water, vitamins, and some minerals while excluding everything else. Partial fasting may include some foods. Anyhow, all types of fasting share the same idea of drastically reducing food intake.
Fasting reduces fat by about 1 lb. (500g) per day. We require quite a bit of energy just to maintain our body temperature and basic biological functions such as pulse and breathing. When there is no food intake, the body takes out the needed energy from the fat previously stored. Therefore, fasting may look like a very effective weight loss method if we just look at short-term weight reduction. However, it is not that simple. Fasting is very difficult and traumatic on your body. Also, fasting severely curtails your energy levels making it almost impossible to perform daily activities. The most serious side effect of fasting is it often destroys our normal energy metabolism. This destruction works as follows. When you begin to fast your body’s metabolism reacts by slowing down and trying to conserve the present fat storage. Even after fasting, your body’s basic metabolism does not return to normal for some time. Therefore, after a fast people tend to gain back all the weight lost at even a faster pace because their slow metabolism is not burning off the normal amount of calories. This process can be compared to people who have experienced financial difficulties. They begin to conserve their pennies and save more. Fasting is similar; the body becomes more efficient at saving calories to add on new fat deposits. Almost always the weight lost comes back very quickly. Most of the weight loss achieved during the fasting period comes back within two to three weeks even with normal eating. Remember the body is desperately trying to store energy since it has been fooled into believing there is a lack of food available for consumption. In most cases, obesity levels after fasting are more serious than pre fasting levels. The body’s basic metabolism has been altered and it is more prone to adding weight. The capacity to burn calories is severely damaged.
Due to the physical and mental strain of a fast, a serious fast may lead to a serious depression. This state of depression may cause individuals to overeat after fasting. Fasting may also cause permanent damage upon key organs due to the lack of nutrition consumed during the fast. Considering all these points, we do not recommend fasting as a suitable weight loss method.
2) Selective Diet
After fasting, the next weight control method is maintaining a selective diet. That is, eating smaller portions of select things. For example, if the daily intake of calories is reduced to 1000cal, weight can be reduced by 8-10kg in the first month and 15-20kg in the next three months. Two popular examples of this method is the 멖ollywood 18-day diet?and 멦he Scarsdale Medical Diet? Selective diets also include the one food diet. The one-food diets allow you to eat regular to plentiful amounts but only few kinds of food. A few common examples are the 멐mperor뭩 Diet?which allows you to eat only meat or the 밎rape Diet?where you can consume as many grapes as you like.
Selective diets should be evaluated using the same guidelines that we use to determine a healthy balanced diet. Thus selective diets are normally deficient in one of two ways. First they cause a disruption in our basic metabolic system, because like fasting they drastically reduce our food intake. The body’s reaction is always the same ?it slows our metabolism further. This causes future weight gain to be even larger. Second, these selective diets can cause a malnutrition problem because your diet is no longer properly balanced. Eating all the meat that you want may sound appealing to the dieter but it will cause a nutrition imbalance. The body뭩 cells will react to this nutrition imbalance by demanding further food. This will eventually lead to additional eating. We are not suggesting all these selective diets are harmful to you, however, please be careful. They can be very similar to fasting methods and leave permanent changes on your basic metabolism that will lead to long-term weight concerns.
3) Medication (pills and drugs)
Some people use drugs to control their weight. There are drugs which suppress appetite, drugs that act as diuretics, and drugs for many other purposes. When taking any drug you should always be concerned about side effects and dependency.
Here are a few of the most common drug groups that suppress a person뭩 appetite:
1) Catecholamine is sold under the brand names Phenthermine, Mazindol, Diethylpropion and Phenylpropanolamine. The Catecholamine drug group works by stimulating the 몊atisfaction?nerves in our brain or by numbing our 멲ppetite?nerves. As side effects, this drug group raises a person뭩 blood pressure and may cause an irregular pulse.
2) Serotonon is sold under the brand names DL-fenflurammine, Dexfenflurammine, Fluoxetine, or Fluvoxamine. The Serotonon drug group stimulates the secretion of Serotonin which increases the feeling of fullness. On the average, these drugs tend to decrease meal sizes by 15%. The side effects of this medication are sedation and low blood pressure.
3)PhenFen is also known to reduce appetite. It was very popular in the North America but it has now been shown to have serious side effects on the heart.
There are also drugs that act as diuretic agents to stimulate urination. Healthy urination is vital to the body because it secretes all kinds of accumulated wastes out of the system. Urination is the body뭩 cleansing system. Most medicinal herbs contain diuretic ingredients. Diuretics are often used to treat high blood pressure and swellings from high blood pressure and kidney diseases. Also, most diuretic agents are known to have some weight controlling effects. Some diuretic agents produce weight loss by reducing only the amount of water in the body, and some agents remove other things too. It is natural to consider diuretic agents as a method to control weight.
However, there are many kinds of diuretic agents. If too much or the wrong diuretic agents are taken, the body develops certain resistance toward the specific diuretic stimulation. Also, the body starts to depend on diuretic stimulation even for normal urination. Our bodies are known to develop resistance to all chemical diuretic agents. Also, chemical diuretic agents are known to have other serious side effects. Some key nutrients also go out of the body in the diuretic process, occasionally resulting in malnutrition. Therefore, we have to be careful before using diuretic agents for weight control. Weight loss that results from diuretics is mostly temporary water lose, anyway. Weight loss incurred by diuretic agents certainly comes back quickly. However, diuretic agents are very important and valuable tools for many purposes, but can not be relied upon as a means of safe and permanent weight control.
Recently, there have been a few popular drugs for weight loss. One of them is called Xenical, a drug marketed by Hoffmann-La Roche. Xenical has been a tremendous success of the pharmaceutical industry. It claims to be the first 몁on systemic lipase inhibitor? This means that it prevents the body from absorbing fat. This is a fantastic claim, but it is still a new product. We need more time to really evaluate this product. According to Dr. Morton Maxwell at UCLA뭩 Obesity Center, only one third of the users have seen positive effects. It is also expensive – $4-5 dollars for a day뭩 dosage. It can cause nausea. Xenical is a prescript-xion drug. We believe that once the body is accustomed to Xenical, the body will become dependent upon Xenical for handling fat. The body뭩 metabolism will also be reduced and the individual will become more obesity prone. As its known effects are still short term ones, we will have to continue to monitor this drug.
Cellasene is another recent commercial success. In some countries, it is not considered a drug and sold as a dietary supplement. It is made of a few herbs that have a well-known efficacy to help the circulation of the capillaries. One of these herbs is Ginko Biloba. It should be taken three times a day for eight weeks. After this it should be taken one time per day for maintenance. Cellasene claims to tighten up those lose fat parts on the hip and thigh areas. But, it does not control weight. It just tightens up those loose areas. The manufacturer stresses, 뱘ou may not lose weight, but you will lose inches? Some doctors who have used it say that it actually does make people lose inches in just four weeks. Side effects such as dry mouth have been reported. This product does not stress weight loss but instead becoming more compact or losing inches.
Well, you will hear about several new kinds of drug products every year. Some of them may be good while most usually have long term side effects. Later in this booklet, we explain some guidelines to determine which of these 몏onder drugs?and 몀iracle treatments?are truly sensible weight loss methods.
4) Herbal Products and Dietary Supplements
Recently, various Chinese herbal medicines have been introduced to western countries. Chinese herbal medicines claim to be different from western pharmaceutical drugs. They claim to work on the whole human body. Thus their goal is to improve a person뭩 general health while treating obesity. Many Chinese herbal medicines claim that they are free from side effects because they are made from natural plants.
We agree with the goals of Chinese herbal medicine. A person뭩 general metabolic condition must be improved if we are to properly treat obesity. This requires a whole body approach. However, we emphasize that all the claims of these Chinese herbal medicines should be reviewed carefully. For example, being 몁atural?itself does not guarantee safety. There are many natural substances that are quite dangerous. Also when a product is produced in China there is a concern about the lack of quality control. One should investigate 1) whether any herbs are contaminated by herbicides, pesticides or chemical fertilizers 2) whether the Chinese herbal medicine was manufactured under the correct environment and scientific controls and 3) whether the herbs listed are truly what is being provided. One extreme example is that a small percentage of Chinese medicinal herbs have been shown to contain traces of herbs such as Mahuang (Ephedra). Mahuang is known to be a strong narcotic.
Some Chinese herbal medicines used for weight control contain the aforementioned Mahuang and other herbs whose narcotic ingredients heighten metabolism. Increased metabolism stimulated by narcotic agents will surely lead to weight reduction. But, this is obviously not a healthy method of weight control.
Some countries put these herbal medicines on their black lists. The side effects can be quite severe, like causing permanent kidney and liver damage. It is wrong to believe that something is 몊afe?because people say that the product is 몁atural?
Another group of herbal products, which deserve comments are 몋hermogenic?products which are based on herbal extracts such as Guggulipid, Fucus, Cola Nut, and Ginger. The name 몋hermogenic?stands for the herb뭩 ability to raise body temperature. The way these herbal products work is by changing how the thyroid gland works. We have indicated already that changing the hormonal balance of a person in general may be dangerous. Even though this particular hormonal change was not yet extensively studied, changing how this thyroid functions may have very serious long-term side effects. The brand names of this 몋hermogenic뭛roup are Thyrolean, TLN, Natural Balance, Reduce 7 in 1, and Metabolean.
Other herbal products and dietary supplements have some weight control effects, simply because they block the digestion process. Some work because they induce diarrhea and others induce constipation. Some make food expand inside the stomach. Some claim that they assist the coagulation of fats and then these fats leave the body. All of these products have side effects. As long as these products fail to address the basic metabolic problem (the vicious cycle of obesity), these products effect will only be temporary. Temporary effects but your body may be exposed to several dangerous side effects.
5) Weight Loss Machines
Steam sauna boxes, motorized massage machines, electronic muscle stimulating machines, etc. are constantly being promoted on TV뭩 shopping channels. Again, fancy names are very common – the Fitsizers, Enercisers, Abbusters, Metabosizers are just a few. These products?promises are also common: ? minutes a day, will loss you 10 pounds a month? If these machines would actually build up your muscle mass then they might really burn off the fat they promised. The increased muscle cells will demand additional blood sugar fuel, this will reduce a person뭩 fat level as long as they maintain a steady diet.
However ? minutes a day?will never create enough new muscle mass to reduce ?0 pounds a month? Increasing your muscle mass does not happen this easily. Metabolism changes do not happen like that, either. Tummies do not go away in 5 minutes either. We do not wish to discourage anyone from exercising, even if it is just 5 minutes per day. Some of these products can be quite helpful. We recommend those machines which actually allow smooth and well regulated aerobic exercises (bike machines, treadmills, cross-country ski machines). Remember, as with all exercise programs, you must approach them in a positive and consistent manner. Or else, your exercise machines will only collect dust and become a worthless piece of equipment.
6) Surgical Procedures
We feel strongly that nothing positive can be said about surgical procedures. They can be extremely damaging to your body in the long run. In sum, they are also expensive, painful and permanently harmful. Having indicated our opinion, let뭩 describe briefly some of your surgical options:
1) Vertical Section of Stomach: This operation makes the stomach smaller by cutting the stomach vertically.
2) Stomach Stapling: The stomach and the upper intestines are stapled together to prevent the absorption of nutrients in the small intestines.
3) Jaw Wiring: This operation makes food intake more difficult by binding up the chin and allowing food intake only through a straw.
4) Liposuction: Suction of the body fat using a thin tube. Of the surgical methods, this is most popular because in theory the problematic fat areas can be removed separately and instantly.
Once again, our biggest problem with these surgical procedures is they do not address the metabolic problem. Stapling and making the stomach smaller is a very harsh reaction to stopping overeating. So is jar wiring. Over time the stomach expands as the body craves more fuel and nutrients as it is being staved by this restrictive diet. The surgeons understand this but hope that the person loses a great deal of weight in the initial weeks. We have already described how dangerous liposuction can be. These surgical methods should be used only for extreme cases.
Criteria for Judging Sensible Weight Control Methods
As the obesity problem is a global problem, we will hear about many novel weight control methods. We must always be in a position to know how to evaluate these methods. In this section, we introduce a few criteria to properly evaluate these methods.
We should not chose a weight control method by looking at just one criteria ?weight loss. We must be informed and evaluate all methods by several key criteria. The true objective of weight control is recovering a healthy body metabolism as this will lead to weight loss and looking and feeling better. Weight loss is just a measurement one small indicator of how we are progressing toward this objective. If we keep this in perspective, then it is possible to make the right weight loss choice. Generally, a sensible weight control method should meet the following seven requirements.
1) Whole Body Approach ?The method should be effective on the whole body, as opposed to concentrating on only a few parts. In other words, if some methods promise that certain parts of our body only will be affected, we should be more skeptical. Side effects are more likely as the method focuses on one region. Obesity is a problem that effects a person뭩 whole body and so the solution must address the whole body. If it only addresses a certain area of the body you should expect a limited or temporary weight loss effect.
2) Basic Metabolic Normalization – They should improve and normalize the body뭩 overall basic metabolism. This is the central theme of this booklet. Otherwise, the method is considered cosmetic or plain harmful to the long-term health of the individual.
3) Pain & Effect on Outlook ?The method should be low in pain. There is no reason why for most people this problem needs to be treated in a manner that involves a great deal of pain. The Method should not cause depression or have a large negative effect on the person뭩 outlook.
4) Lack of Side Effects – There should be no side effects. The method should be safe. Toxicity and other contaminants like herbicides, insecticides and chemical fertilizers should be monitored closely. Remember even if it is a natural product it may not be safe.
5) No Resistance or Dependence ?The method should not cause either resistance or dependence to be developed. We should avoid all methods which induce the body to become dependent upon something unnatural on a permanent basis. In the above sections, we gave a few examples of these drug dependent situations. In obesity cases, when a person뭩 metabolism becomes dependent upon a drug, this leaves the body permanently in need of this drug. As the body, in turn, becomes more resistant to this drug the person begins to need additional quantities. For example, if the diuretic agents are used too much, such a vital biological function as urination becomes dependent upon a drug. The long-term consequences of the unnecessary dependence can be quite severe.
6) Long-Term in Nature ?The methods should result in long-term weight loss and control. Once some weight is lost, it should stay lost at least for a long time and hopefully permanently. Short-term fluctuation of weight is not healthy. Sensible weight control methods should enhance the level of metabolism to a higher state, then, the weight control effects will stay for the long term. Otherwise, weight control effects are short-lived.
7) Convenience ?The method should be relatively easy to acquire and use.
We believe that there are sensible weight control methods that meet all the above seven criteria.
CHAPTER 4: A Sensible Combination of Four Weight Control Methods
Considering all the side effects, the other shortcomings of various weight control methods, and the fact that the re-normalizing the metabolic balance is at the core of the problem, we believe that obesity should be attacked with the combination of all of the following 4 methods:
1) Stress Management
2) Healthy Eating Habits
3) Regular Exercise and
4) Metabolism Boosting Dietary Supplement
Let뭩 examine each one more closely.
Stress Management
People tend to compensate for their stressful lives by finding different ways to relieve their stress. Some listen to music and some watch a movie. Some relieve their stress by having long conversations with their friends, and others believe in exercise. However, it is quite common that one way an overweight individual will respond to stress is by overeating.
Therefore, stress management is the first sensible thing one should do in order to fight obesity. In this regard, many proven relaxation techniques have been developed. Please review the ten relaxation techniques listed below and try to select two or three that will work for you. Stress is a major cause of numerous problems, we should all take steps to improve how we deal with stress as this will definitely improve our lives.
Stress Reducing Techniques:
1) Imagination ?Imagine a beautiful, comfortable and relaxing scenery or, situation.
2) Meditation ?Close yourself from all external interruptions and concentrate only on one peaceful subject.
3) Biofeedback ?Learn to take conscious control of the body뭩 inner physiological variables such as heart beat, blood pressure, skin temperature. Listen to your heart-beating and breathing and feel the calm it brings over your body.
4) Progressive Muscle Relaxation ?Lying down in a comfortable position, start flexing and then relaxing your various body-parts in a sequential manner. Start with one leg and move around the whole body.
5) Breathing Exercises – Concentrate on controlling the pace of your breathing. In a seated or laid position, start to relax by varying your breathing patterns from slow and deep to normal and shallow.
6) Aromatherapy – Relaxing your tension by using fragrances like roses and apple fragrance. Fragrances can be used to increase the pleasure and relaxation of a bath or for massage therapy.
7) Massage Therapy ?Practice makes perfect when it comes to becoming an effective masseuse or if you want to learn the basics take a couples massage class. This is a great way to relieve tension.
8) HydroTherapy ?Try floating in relaxing warm water.
9) Music Therapy – Use music to relax you and help you drift away.
10) Self-Hypnosis ?The repetition of self-motivating phrases or beliefs.
All the above relaxation techniques are quite well known and relatively safe. Fortunately, there are many qualified professionals who can help you learn and master your favorite relaxation techniques. They are also not that expensive. These relaxation techniques not only help you to control weight they provide many other health benefits. So make relaxation your first weight loss technique and we believe you will be pleasantly surprised.
Healthy Eating Habits
As we have said fasting or having an extremely low calorie diet that lacks nutritional balance is not a sensible means to control weight. Eating sensibly and properly is what brings the desired long-term results. Fortunately, eating sensibly is a well-developed subject that has a high level of public awareness and knowledge. Most people understand that they must regulate both the quality and the quantity of food consumed. We also know that a balanced diet, one that covers all four-food groups, is preferred. As there is many sources from which people can get the valuable information about this issue, we have not elaborated on this topic. However, this must be a key component of every sensible weight loss program.
Regular Exercise
Exercise has a direct effect on reducing a person뭩 body fat and blood sugar surplus. Regular exercises also stimulates the metabolism and revitalizes the production of insulin. An increased metabolism and insulin circulation in the blood stream will boost blood sugar consumption or processing, and improve insulin sensitivity. Exercise, any kind of increased movement, is extremely beneficial. Like healthy eating, there is so much great literature on the benefits of exercise, that we will just add a few comments.
For obesity patients, we recommend exercises that involve the whole body and are low in intensity level so that the person can maintain the exercise for over 30 minutes. Light exercises such as, walking, jogging, cycling, cross-country skiing, and easy mountain climbing are ideal. The goal is try and use all the major muscle groups so that the person slowly develops more muscle mass. Severely obese people should consult with their doctor to find a suitable exercise program. Consistency and developing a daily routine that makes exercise a top priority must be your goal.
One last thing about regular exercise as a weight control method. We recommend that you stay away from swimming if you can. Swimming is not as helpful in reducing weight as many believe. When you body is consistently in relatively cold water, it develops a defensive system against this cold. This defensive system is a layer of fat. Also since the body is floating in water when you swim, the effect of gravity is not as strong as during other exercises. This results the person burning fewer calories. This reduces the weight loss efficiency of swimming. Also, swimming has been shown to increase the appetite. So unless, your swimming is very vigorous, we would recommend another fitness exercise.
Metabolism Boosting Dietary Supplement
The above three methods (stress management, healthy eating habits, and proper exercise) are very fundamentally sound weight control methods. Unless poorly done, they do not have side effects. They also address the core of the obesity problem ?the metabolism imbalance. Stress management techniques assist an individual to avoid dangerous overeating that can result from their reaction to high stress levels. A balanced diet is essential to ensure intake of food calories is balanced with energy consumption. Physical fitness and exercise increases the muscle mass of the body thus increasing the metabolism. Thus all three methods are effective, safe and sound components to any weight loss program.
However, they do not seem to be enough. If they were enough, you would not be reading this booklet. These weight control methods have been known for a long time. If they were sufficiently effective, then the obesity problem would not be escalating through out the world. We suspect that the above methods are truly effective only during the initial stage of obesity. However they are not so effective during severe stages of obesity. When the basic energy metabolism itself is in a wrong cycle or during a later stage of obesity, the above three methods are not enough. In other words, the above three weight control methods are good enough for healthy people to maintain a healthy metabolism and they will also help control cases where people are mildly overweight. But, once the vicious cycle of obesity sets in, the above three methods alone are not sufficient to stop this cycle. In such cases, the above three methods should be assisted by metabolism booster which is both safe from side effects and effective. Eleotin-Mb is such a product. In Chapter 5, we will provide a brief history of this product and review how Eleotin-Mb works to provide a long-term weight loss solution.